
Author: Anna Gardin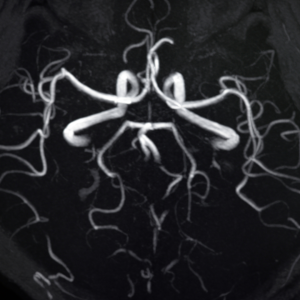
Stroke Unit, Clinical and Experimental Medicine Department, University Hospital “G. Martino”, Messina, Italy
Twitter:@AnnaGardin1
Intracranial arterial dolichoectasia (IADE) is defined as an increase in the diameter and length of at least one intracranial artery. This pathology affects the posterior circulation in 80% of cases, causing a malformation of the basilar artery, which is showed elongated, dilatated and often tortuous.1 This vascular alteration is particularly relevant because it seems to be related to a higher risk of stroke and it is found in about 12% of stroke patients.1
To date, the diagnostic criteria are not clearly established, mostly because of insufficient data about the cutoffs between normal and pathological dilatation and elongation of intracranial arteries. Smoker and colleagues well defined these aspects for the basilar artery and their criteria are recognised as having a good accuracy value in the diagnosis of basilar dolichoectasia. Therefore, a basilar artery is defined as dilated with a diameter greater than 4,5 mm on MRI axial sections, while it is elongated if it crossed over to the margin of the dorsum sellae or if its bifurcation was above the plane of the suprasellar cistern. 2 On the contrary, no validated criteria are available for the anterior circulation.
Differently from the atherosclerotic process, which is caused by the infiltration of inflammatory cells and lipidic cells in the arterial wall intima, IADE involves the tunica media and the internal elastic lamina, with impairment of extracellular matrix (ECM) and smooth muscle cells. In patients with IADE, modifications of ECM may be the result of an imbalanced matrix metalloproteinases (MMP) activity, particularly demonstrated by lower MMP-3 plasma concentrations. Similarly, MMP-3 levels are associated with ectasia of coronary arteries.3 Metabolic disorders involving smooth muscle cells (e.g. Pompe’s disease, Fabry’s disease) or elastic fibres (e.g. Marfan’s syndrome, mutations in the collagen IV alpha 1 or 2 genes) also can be associated with IADE. Specifically, in Fabry’s and Pompe’s disease, the lipid accumulation in endothelial and smooth muscle cells weakens the arterial wall leading to tortuosity and dilatation.
The main neurological manifestations of IADE are ischaemic stroke or transient ischaemic attack (34%), compression of surrounding structures (cranial nerve/brainstem/third ventricle with hydrocephalus) (28%), and intracerebral haemorrhage or subarachnoid haemorrhage (7%).4 IADE is also correlated with systemic arterial dilatations, like enlarged descending thoracic aorta, abdominal aortic aneurysm, saccular aneurysm, and coronary artery ectasia.
An interesting work by Del Brutto and colleagues has tried to clarify the clinical correlates of IADE and acute ischaemic stroke. IADE is likely responsible for a percentage of strokes initially categorised as of undetermined aetiology or as related to small-artery occlusion.5 Supporting that, IADE is demonstrated to be linked to lacunar infarcts, in particular at pons, where perforating arteries arising from the dolichoectatic basilar artery could be occluded by vessel distortion or intraluminal thrombus formation. In addition, several studies have highlighted the possible correlation between IADE and cerebral small vessel disease. These two entities may share the previously exposed pathophysiologic models based on MMP dysregulation and genetic mutations.6
In conclusion, a considerable part of stroke cases may be due to IADE (the prevalence ranges from 3 to 17%7), which should be considered in the diagnostic workup. Surely, further studies are necessary to better establish the diagnostic criteria. Moreover, because of the link with different pathologies (e.g. cardiac infarction, aortic aneurysm, metabolic and genetic diseases), when IADE is suspected, it is important to screen the patient for relevant comorbidities to find the best therapeutic approach.
—
References
- Pico F, Labreuche J, Amarenco P. Pathophysiology, presentation, prognosis, and management of intracranial arterial dolichoectasia. Lancet Neurol. 2015 Aug;14(8):833-845. doi: 10.1016/S1474-4422(15)00089-7. PMID: 26194931
- Smoker WR, Price MJ, Keyes WD, Corbett JJ, Gentry LR. High-resolution computed tomography of the basilar artery: 1. Normal size and position. AJNR Am J Neuroradiol. 1986 Jan-Feb;7(1):55-60. PMID: 3082144; PMCID: PMC8334772.
- Pico F, Jacob MP, Labreuche J, Soufir N, Touboul PJ, Benessiano J, Cambien F, Grandchamp B, Michel JB, Amarenco P. Matrix metalloproteinase-3 and intracranial arterial dolichoectasia. Ann Neurol. 2010 Apr;67(4):508-15. doi: 10.1002/ana.21922. PMID: 20437586.
- Shapiro M, Becske T, Riina HA, Raz E, Zumofen D, Nelson PK. Non-saccular vertebrobasilar aneurysms and dolichoectasia: a systematic literature review. J Neurointerv Surg. 2014 Jun;6(5):389-93. doi: 10.1136/neurintsurg-2013-010793. Epub 2013 Jul 10. PMID: 23843444.
- Del Brutto VJ, Gutierrez J, Goryawala MZ, Sacco RL, Rundek T, Romano JG. Prevalence and Clinical Correlates of Intracranial Dolichoectasia in Individuals With Ischaemic Stroke. Stroke. 2021 Jul;52(7):2311-2318. doi: 10.1161/STROKEAHA.120.032225. Epub 2021 May 13. PMID: 33980042; PMCID: PMC8238812.
- Zhang DP, Yin S, Zhang HL, Li D, Song B, Liang JX. Association between Intracranial Arterial Dolichoectasia and Cerebral Small Vessel Disease and Its Underlying Mechanisms. J Stroke. 2020 May;22(2):173-184. doi: 10.5853/jos.2019.02985. Epub 2020 May 31. PMID: 32635683; PMCID: PMC7341005.
- Del Brutto VJ, Ortiz JG, Biller J. Intracranial Arterial Dolichoectasia. Front Neurol. 2017 Jul 17;8:344. doi: 10.3389/fneur.2017.00344. PMID: 28769872; PMCID: PMC5511833
ESOC is Europe’s leading forum for advances in research and clinical care of patients with cerebrovascular diseases. ESOC 2023 will live up to its expectation, and present to you a packed, high quality scientific programme including major clinical trials, state-of-the-art seminars, educational workshops, scientific communications of the latest research, and debates about current controversies. ESOC 2023 programme is now available, and registration is open. Learn more here.
